Published: April 16, 2026 | ORIGINAL RESEARCH | RRMJournal.org
Public Awareness, Perceptions, and Preferences in Fertility Treatment:Secondary Analysis of Two Public Surveys
Tracy Parnell1,2, Kathleen Copeland1, Monica Minjeur1,3
1International Institute for Restorative Reproductive Medicine, Crawley, West Sussex, UK; 2Department of Family Medicine,University of British Columbia, Vancouver, BC, Canada,;3Radiant Clinic, Cedar Rapids, IA, USA
https://doi.org/10.63264/6yy3mw82
ABSTRACT
Objective: This study examined public attitudes toward restorative reproductive medicine (RRM) and in vitro fertilization (IVF) using secondary analysis and comparative reporting of two independent surveys conducted in theUnited States. It also explored preferences among individuals with fertility issues and the general population’s views on treatment options.
Method: A secondary analysis was conducted using data from two nationally representative online surveys, designed and administered by organizations independent of the researchers, whose samples demographically reflected the U.S. adult population. The surveys conducted by J.L. Partners (N=1002) and McLaughlin & Associates (N=1000)—assessed familiarity, acceptance, and attitudes toward IVF and RRM. The J.L. Partners survey focused on IVF, including medical risks, creation and use of embryos, preimplantation genetic testing, arguments for government oversight of IVF, and overall attitudes toward IVF. The McLaughlin survey focused on comparative descriptions of IVF and RRM. Pearson’s Chi-Square tests of independence were used to assess differences in response distributionsacross demographic subgroups and between survey items of interest.
Findings: Overall, there was strong consistency of responses to items that were similar in the two surveys. Approximately 80% supported IVF initially, although both surveys found respondents to have limited knowledge about IVF procedures. In contrast, 33% supported RRM initially, with 43% having never heard of RRM. After learning more about the characteristics of RRM and IVF approaches, as presented within the surveys, preference shifted toward approaches consistent with RRM (e.g., 69% preference for an approach for natural fertilization in a woman’s body vs. 17% for fertilization in a lab). Respondents prioritized baby health (74%) over cost (13%) and time to conceive (6%). Many IVF patients were concerned about undiagnosed health issues and being rushed into IVF. Overall, 70% wanted treatments that addressed underlying causes; nearly half were unaware of any medical risks of IVF. Stated support for IVF declined by 10% overall after presentation of medical risks, questions about the creation and use of embryos and genetic testing, and arguments to support government oversight of IVF. Both surveys showed strong support for patient access to full information about treatments and treatment processes
Conclusion: While IVF is widely accepted, these national survey data suggest preferences for fertility treatments that prioritize diagnosis and restoration of natural reproductive health, which is the focus of restorative reproductive medicine. Comprehensive assessment, restoration of healthy function, transparency regarding treatment processes, and sensitivity to ethical concerns in patient care reflect important public values. Greater awareness and public education, improved consent, more research, and ongoing surveys are needed to inform public health strategies and meet patient needs in fertility care.
Keywords: infertility; fertilization in vitro; public opinion; restorative reproductive medicine; delivery of health care; reproductive medicine
INTRODUCTION
Infertility is generally accepted to be the failure to conceive after 6-12 months of regular unprotected intercourse, with the timeframe varying by age.1 Infertility is not a singular disease entity, but is often a symptom of underlying dysfunction, and it remains a critical public health issue in the United States and globally.2 The total fertility rate in the U.S. is currently 1.57 births per woman, below the replacement level of 2.1, raising concerns about long-term population sustainability and potential socioeconomic impacts.3, 4 In addition to population-level considerations, fertility challenges impose substantial emotional, physical, and financial burdens on individuals and families, underscoring the need for ongoing attention and targeted interventions.5
Perhaps the most prominently discussed treatment developed for infertility is in vitro fertilization (IVF), which refers to a method whereby eggs are fertilized with sperm outside the human body in a laboratory, with the intent to transplant a developing embryo back into the human body.6 IVF was pioneered in the late 1970s, with the first successful birth in 1978, and has seen a dramatic increase in utilization since 19837 with an estimated 9.8–13 million children conceived through IVF born worldwide.8, 9 IVF uses many different protocols to assist in harvesting eggs; nearly all these techniques require giving or inducing very high levels of reproductive hormones to allow for simultaneous harvesting of multiple eggs. These eggs are then frozen or processed for fertilization. An additional term that is often used to refer toIVF is assisted reproductive technology (ART). While the term ART may include several types of fertility treatment, it is usually applied to IVF and closely related procedures.
In the year 2000, restorative reproductive medicine (RRM) was defined by clinicians and researchers as a field of medicine that focuses on diagnosing underlying factors causing or contributing to reproductive dysfunction and infertility and then treating these underlying factors to correct or improve reproductive function.10 As a supportive and restorative approach, RRM prioritizes natural, healthy physiology. RRM takes a classic medical approach to the treatment of infertility, diagnosing and treating contributory pathology, using principles of chronic disease management as a strategy for improving long-term health.11 Published data report RRM live birth outcomes comparable to IVF,12 and some studies report fewer of the complications associated with IVF including multiple gestations, premature birth, and low birthweight.11, 13, 14.
With infertility rates rising and fertility care services rapidly changing, it is important to understand the needs of patients as well as public awareness and acceptance. This secondary analysis looks at two recent surveys that explored these concepts, conducted separately and independently.
METHODS
This study represents a secondary analysis of two independently conducted surveys. While the original surveys were funded and designed by external organizations, the current analysis was conducted independently by the authors, without involvement from the originating organizations.
The first survey was conducted by J.L. Partners (JLP) between March 31 and April 3, 2025, using an online polling platform with sampling to ensure geographically representative data; it explored Americans’ knowledge of and opinions about IVF. The 1,002 registered voter respondents also had data collected regarding 2024 presidential voting, partisan identification, age, ethnicity, gender, education and population density. The margin of error was +/-3.4%. The survey investigated attitudes toward medical risks, and embryo storage, preimplantation genetic testing, and government oversight of IVF. It also asked about hypothetical alternatives to address underlying causes of infertility, but did not use the term RRM.
The second survey was conducted between April 26 and May 4, 2025, by McLaughlin & Associates (McL). Individuals were invited by email to participate in the online survey, from a pre-populated polling panel with diverse representation, recruited from online advertisements and outreach. Randomly distributed invitations ensured demographic and geographic representativeness of the 1,000 respondents aged 25-60. The margin of error was +/- 3.1% at a 95% confidence level. Respondents provided information about personal and indirect experiences with infertility and miscarriage, treatment histories, and opinions on reproductive technologies. The survey also collected information on partisan identification, age, ethnicity, gender, education and population density. The survey focused on public awareness and attitudes toward different methods of treating infertility, particularly RRM and IVF. RRM and IVF were named and asked about directly and were also described indirectly and hypothetically for some of the questions, without naming the approach specifically.
This study met the requirements for institutional review board exemption. Ethics review is not required for research that relies exclusively on secondary use of anonymous information, or anonymous human biological materials, so long as the process of data linkage or recording or dissemination of results does not generate identifiable information. Participant information was recorded in such a manner that the human subjects involved cannot be identified.
Questionnaire
The JLP survey is publicly accessible.15 The survey encompassed 32 questions on topics focusing on knowledge about IVF, acceptance of alternatives that focus on restoring function and correcting root cause problems, as well as risks and controversial ethical questions of IVF. Support for IVF was assessed at the beginning and again at the end of the survey.
The McL survey consisted of 55 questions, including standard demographic items and questions regarding ideological or political orientation (22 items).16 While the questionnaire and summary results were publicly available, additional cross-tabulated response counts were obtained from McL for the purposes of statistical analysis.
Statistical Analysis
The analysis focused on two domains:
- Public and patient approval of treatment options, preferences and experiences, which compared IVF and RRM, both directly by name and hypothetically, based on descriptions of the treatment processes. Factors influencing preferences were also explored.
- Knowledge of IVF, attitude toward medical risks, embryo selection and storage, government regulation, and informed consent.
Questionnaire responses were reported using descriptive statistics to summarize frequencies and percentages for each survey item. Chi-square tests were performed to test for select binary outcomes and for repeated questions posed at the start of the JLP survey, and then, after providing further information, at the end of the survey. Many responses were consolidated into three categories: Support (combining “Strongly support” and “Somewhat support”), Oppose (combining “Somewhat oppose” and “Strongly oppose”), and Unsure. Pearson’s Chi-Square tests of independence were used to assess differences in response distributions across demographic subgroups and between survey items of interest. Because individual responses could not be linked across time points from the publicly available data, pre- and post-exposure responses were treated as independent samples for the pre- post- comparison.
Differences were considered statistically significant at p < 0.05, rejecting the null hypothesis of no difference between groups. Statistical analyses were conducted using Python (SciPy and NumPy libraries).
RESULTS
Demographic Characteristics
J.L. Partners (JLP) Survey
This survey was conducted using standardly accepted polling techniques with individuals selected to ensure representative data by region, age, gender, ethnicity, 2024 presidential vote and partisan identification. This survey was accessed publicly, and the specifics of the demographic breakdown are not available. A total of 1,002 respondents completed the survey.
McLaughlin (McL) Survey
A total of 1,000 individuals responded to all questionnaire items representing broad geographic areas of the United States, with the highest representation from the South (39%) and the lowest representation in the East at (17%) with Midwest and West regions making up 21 and 23% respectively.
Among respondents, there were marginally more females than males (52% to 48%), with 84% of respondents identifying as heterosexual, 13% (n=134) as LGBTQ+, and 3% declining to disclose. The age groups were equally distributed throughout the target groups, 25 to 60 years, with a mean age of 42 years. The participants’ stated political affiliations were 39% Democrats, 32% Republican, and 29% Independent/Other. Their self-reported political ideology was moderate (38%), liberal (34%) or conservative (28%). There was a nearly equal split between pro-choice (47%) and pro-life (45%) respondents. The racial breakdown, 64% White, 16% Hispanic/Latino, 13% African American, 5% Asian, as well as political and religious affiliations, and income levels, were reflective of U.S. Census distributions.17
Eighty nine percent (n=892) of 1000 respondents had health care coverage. Twenty two percent had or were currently experiencing infertility (n=216), almost half (n=496) knew family or friends who had experienced or were experiencing infertility, and 19% (n=195) had personally suffered a pregnancy loss.
Ninety-six patients had used IVF, although only 43% of these identified infertility per se as their main reason for using it. Other commonly selected reasons included advanced maternal age, avoiding genetic disorders and selecting for certain traits (Figure 1). Among those who underwent IVF, just over 39% had a healthy baby, with nearly 25% reporting ‘health challenges’ in their IVF outcome.
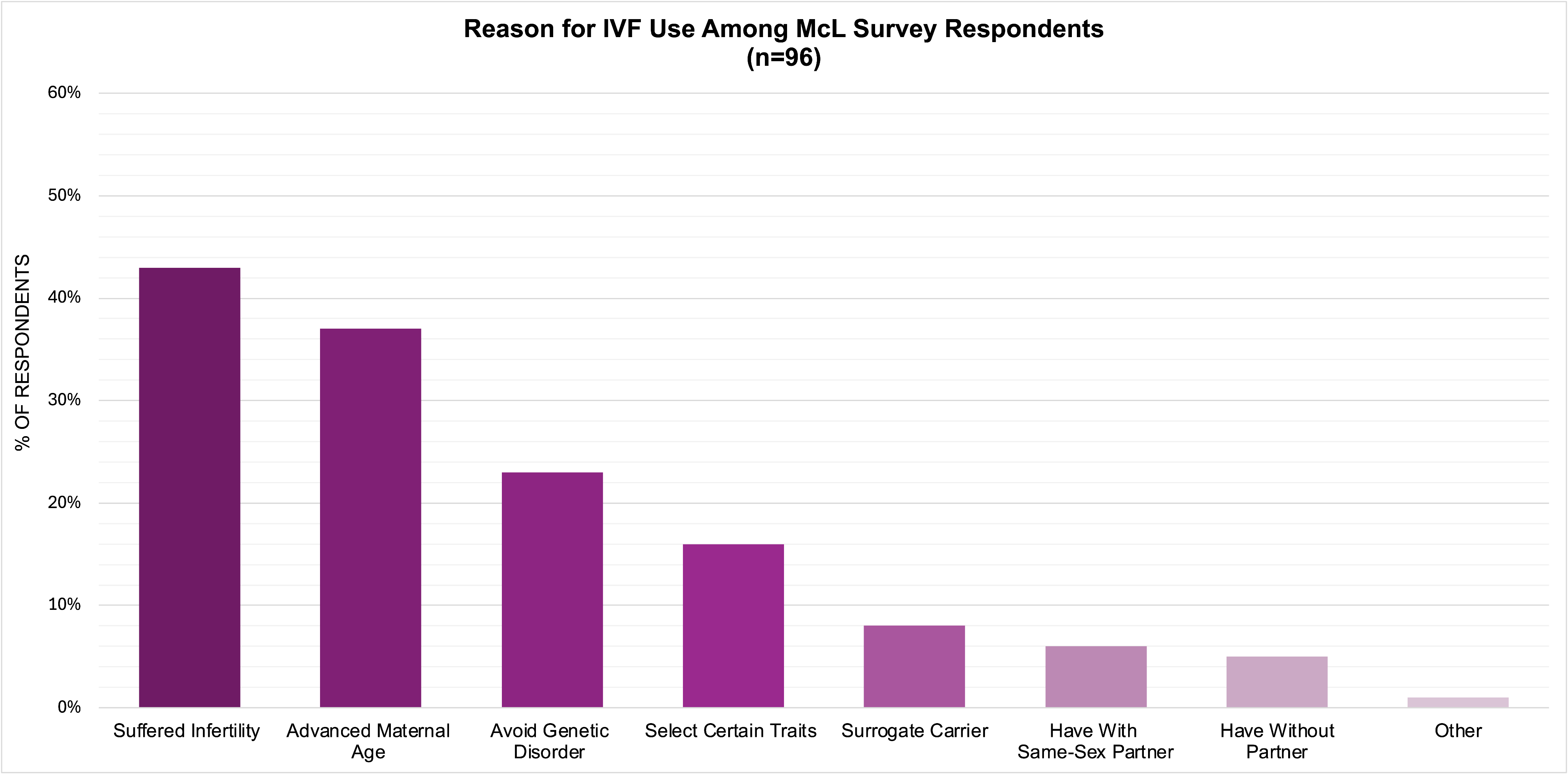
Figure 1. Distribution of self-reported reasons for IVF use among McL survey respondents (n=96).
Demographic Characteristics
Respondents in both groups were overwhelmingly favorable toward IVF at the beginning of both surveys (Figure 2).
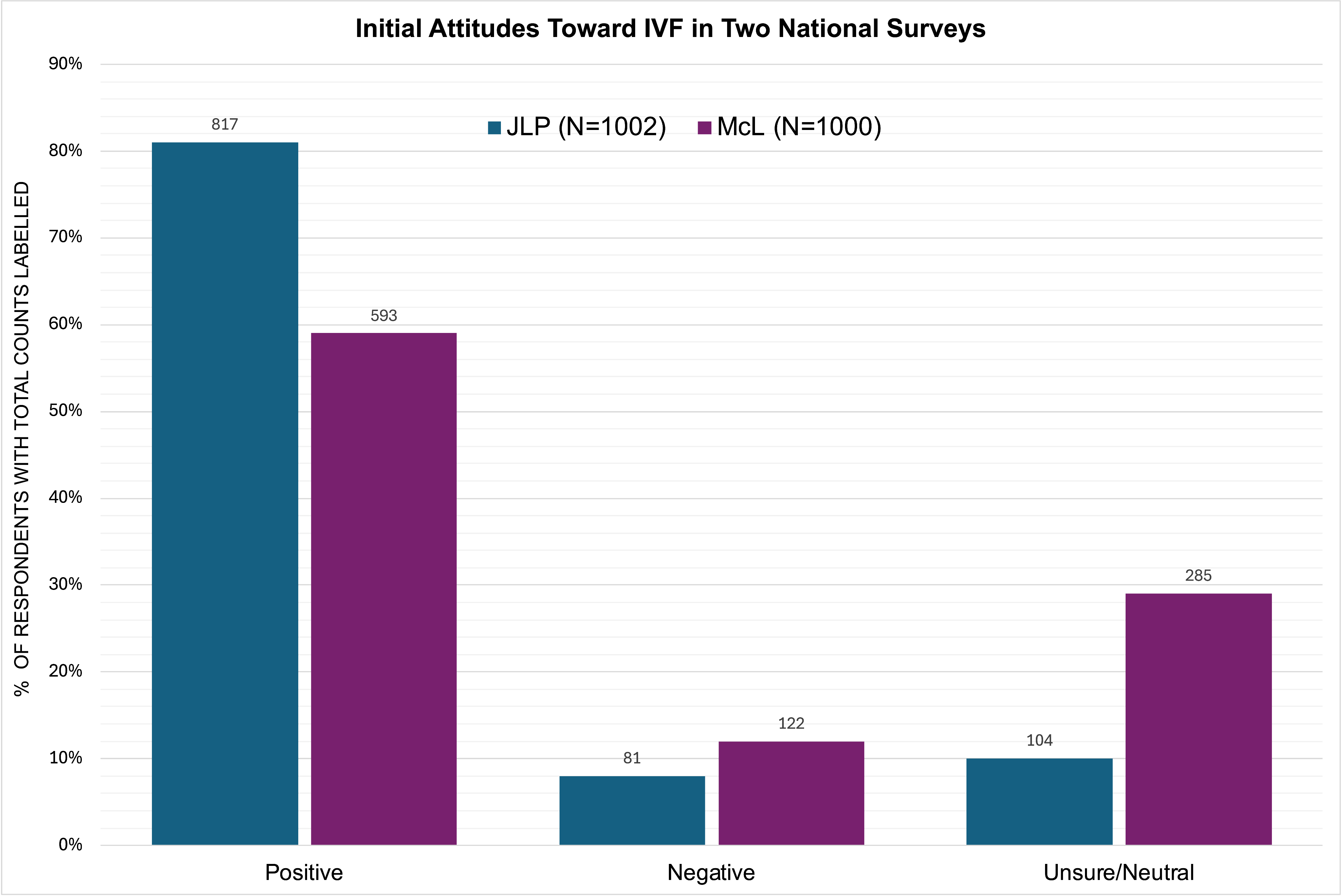
Figure 2. Initial attitudes toward IVF in two national surveys. Because response scales differed between surveys (favorability in McL; support/oppose in JLP), categories were harmonized into three comparable groups: Positive (very/somewhat favorable; strongly/somewhat support), Negative (very/somewhat unfavorable; strongly/somewhat oppose), and Unsure/Neutral (unsure, no opinion, or “never heard”). The “never heard” option was only included in the McL survey for this question.
JLP Survey
At the beginning of the JLP survey, the respondents were initially favorable to IVF with 51% (n=512) strongly supportive and 30% (n=414) somewhat supportive of IVF, 8.0% (n=81) opposed IVF. However, only 14% of respondents (n=145) claimed to be very familiar with IVF, 41% (n=414) were somewhat familiar, 13% were not familiar at all (n=133) and 31% had heard of IVF but knew very little about it (n=310). “Treating the root issue which is causing the symptom of infertility” was preferred over “using IVF as a first line treatment”, 53% (n=531) vs 9% (n=86), with 26% (n=263) choosing a combination of both and 12% (n=159) being unsure.
The question about support for IVF was asked again at the end of the JLP survey. Following exposure to additional information during the survey — including medical risks, embryo storage, preimplantation genetic testing, and several proposed arguments for increased government oversight of IVF (described further below) — the proportion of respondents expressing support for IVF declined 10 percentage points from 81.5% to 71.4%. A chi-square test of independence confirmed a statistically significant shift in the overall distribution of opinions across the categories of Support, Oppose, and Unsure, χ² (2) = 33.28, p < 0.001. The effect size (Cramér’s V = 0.129) indicates a small to moderate shift, indicating that participants became more critical or uncertain about IVF after receiving the additional context presented in the survey. (Figure 3).

Figure 3. Support for IVF Pre and Post Survey (JLP survey). Survey participants (N=1002) were asked at the start and end of survey based on their current knowledge if they support or oppose the use of IVF for couples.
McL Survey
To explore treatment preferences without referring to the names of specific treatments, two hypothetical scenarios were offered in the McL survey meant to represent circumstances relevant to IVF and RRM, but without yet naming any treatments. The hypotheticals were described as follows: “Imagine there are two different solutions for couples with infertility or miscarriage problems: Option A and Option B are equal in all ways except the time it takes to conceive, the cost, and health outcomes. On average, Option A takes less time, but costs more and is more likely to have negative health outcomes for babies, including preterm birth. On average, Option B takes more time, but costs less and has healthier outcomes.” Overall, 68% of respondents preferred option B, with 17% choosing Option A. The preference for option B was 70% in respondents with a history of infertility or miscarriage (n=396). The preference for the two options was similar for respondents who had used IVF (n=96) (Figure 4).
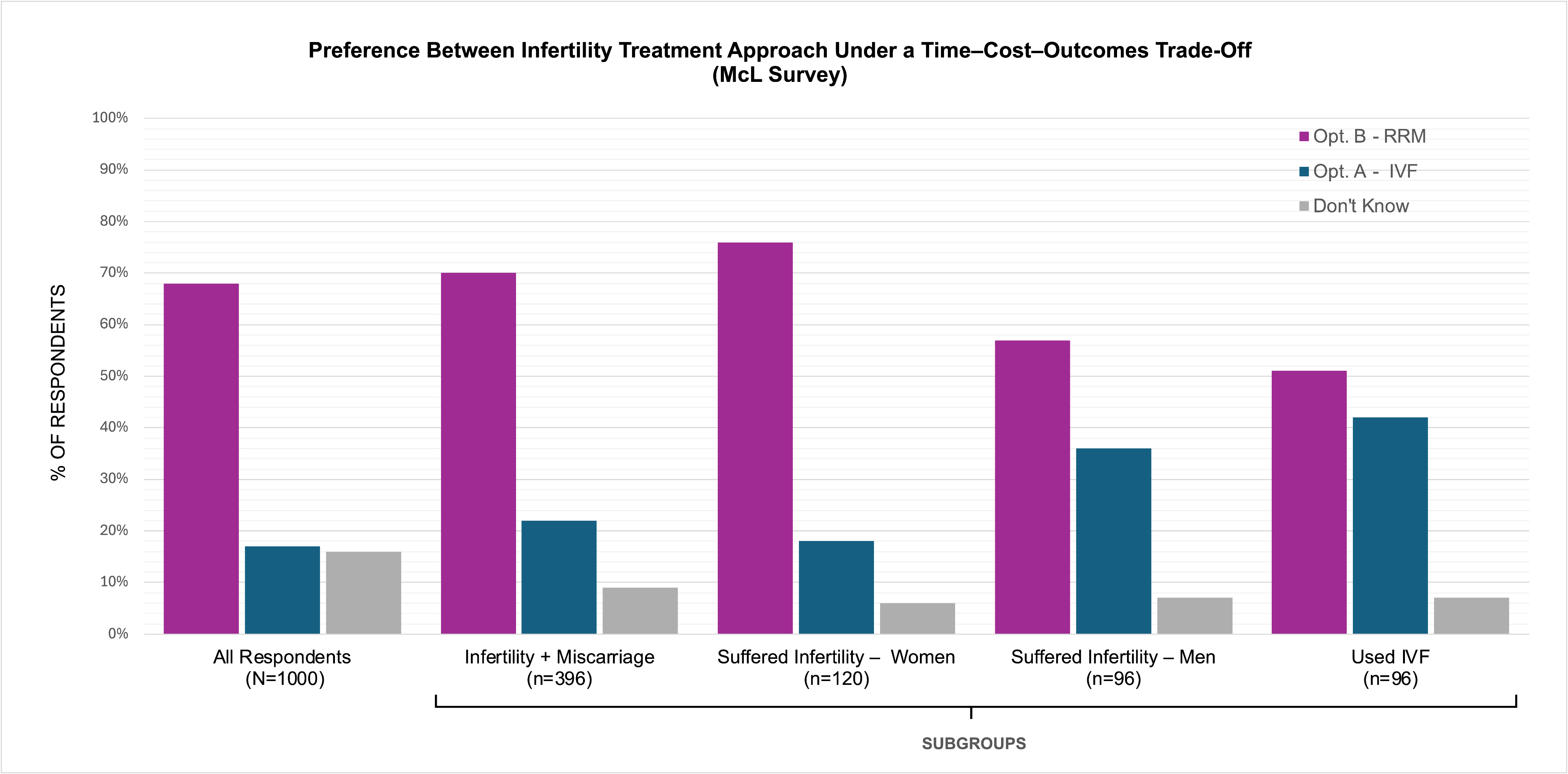
Figure 4. McL survey respondents were posed a hypothetical question for two different solutions for infertility and miscarriage. Option A corresponded to IVF and Option B to RRM: “Option A and Option B are equal in all ways except time to conceive, cost, and health outcomes. Option A takes less time but costs more and is associated with higher risk of negative health outcomes for babies, including preterm birth. Option B takes more time, costs less, and is associated with healthier outcomes. If you were experiencing infertility, which option would you prefer?”. Respondents with infertility/miscarriage experience or prior IVF use are shown alongside results from all survey respondents.
In the second hypothetical scenario, Option X was described as identifying and treating the underlying cause of infertility to allow natural fertilization within a woman’s body, whereas Option Y was described as bypassing the underlying cause and using technology in a lab to support fertilization; pregnancy rates were assumed to be equal. Descriptive analysis indicated that 69% of respondents selected Option X, while 17% preferred Option Y. A Chi-Square test confirmed a statistically significant difference in the distribution of responses, χ² (2) = 573.16, p < 0.05, indicating a greater preference for Option X compared with Option Y (Figure 5).

Figure 5. McL survey respondents were posed a hypothetical question for two different solutions for infertility: “Option X discovers what’s causing the infertility and treats it to support natural fertilization within a woman’s body. Option Y bypasses what’s wrong and uses technology to support fertilization in a lab. Assuming equal pregnancy rates for each approach, if you were in this situation, which option would you prefer?”. Option X corresponded to RRM and Option Y to IVF. Respondents with infertility/miscarriage experience or prior IVF use are shown alongside results from all survey respondents.
This pattern was generally consistent across subgroup analyses. Among respondents with prior IVF use, Option Y (using technology in a lab) was selected more frequently (44%) that in other subgroups; however, Option X (natural fertilization within a woman’s body) remained the most commonly preferred option within this group (52%).
The McL survey next asked participants whether they held favorable opinions on various infertility treatment methods, named before defining them, including IVF, ART and RRM. Just over 59% were favorable of IVF (n=593), with 26% (n=256) being very favorable and 34% (n=338) being somewhat supportive, despite 12% never having heard of it (n=116). The term ART (assisted reproductive technology) was less well known and garnered 37% support overall with 41% having never heard of it (n=406). Slightly over 40% had not heard of restorative reproductive medicine either, while 33% viewed it favorably (Figure 6).

Figure 6. McL Survey respondents were asked their views of IVF, ART and RRM before defining each approach. IVF received the highest favorability (59.3%, n = 593), with 12% (n = 116) having never heard of it. ART was viewed favorably by 37% (n = 370), with 41% (n = 406) reporting no prior awareness. RRM was viewed favorably by 33% (n = 329), while 43% (n = 429) had never heard of it.
After the above questions were asked, the McL defined IVFas, “a process [in which] a woman’s ovaries are hormonally stimulated to produce eggs, and the eggs are surgically removed from her body then combined with sperm in a laboratory to create embryos. An embryo or embryos are then transferred back into her uterus with the aim of pregnancy and a baby. Extra embryos often are frozen for possible future use.” After this definition, overall support for IVF was 79% (n=792), with support lower in patients with a history of miscarriage (73%), African Americans and single men (74%). Support was higher at 85% in LGBTQ+ respondents and 92% in those who had used IVF. (Figure 7, not all data shown).

Figure 7. McL survey respondents were asked to rate their approval of IVF and RRM after brief descriptions of each treatment were provided. Responses are shown overall and by subgroup.
The McL survey defined RRM as, “treatment that focuses on finding and treating the underlying factors causing a couple’s fertility problem that aims to restore reproductive function so patients can conceive and have a baby naturally.” After this definition, approval for RRM was 79% (n=788). Subgroup support was similar for RRM, with 84% of LGBTQ+ respondents expressing approval and 91% of individuals who had previously undergone IVF approving of RRM, with lower rates for single men (74%), African Americans (72%) and higher for those who had a history of miscarriage (81%). (Figure 7, not all data shown).
When given choices about the most important factor to consider in choosing fertility treatment, respondents in the McL survey overwhelmingly ranked the health of the baby as their top priority (74%), followed by cost (13%) and then time to conceive (6%). Men who have experienced infertility and respondents who had undergone IVF, while still ranking health of the baby as most important, reported higher values than others for cost and time to conception, with 45% of those who had used IVF ranking health of the baby as their top priority. (Figure 8).

Figure 8. Most important factors in choosing infertility treatment (McL survey). Respondents selected the most important consideration when choosing a fertility treatment; results are shown overall and by subgroup. Across all groups, the health of the baby was the top priority.
Several of the questions in the McLaughlin survey explored patient treatment experiences, concerns, and other factors that might influence treatment decisions. Overall, 82% of respondents agreed that a comprehensive work-up to identify and understand underlying contributing factors was very important.
Significant concerns were expressed in the survey about undiagnosed health problems contributing to infertility. Among all respondents who reported history of infertility or miscarriage (n=396), 55% were concerned about an undiagnosed health problem. Notably, 83% (n=76) of patients who had undergone IVF felt concerned that there was an undiagnosed factor that contributed to their infertility. A high level of concern was consistent across other subgroups. (Figure 9). Additional patient-experience responses are shown in Figures 10 and 11.

Figure 9. Patient concern about undiagnosed underlying health factors as a cause of their infertility based on a subgroup analysis of McL survey respondents who had experienced, or are experiencing, infertility or miscarriage.

Figure 10. After diagnosis, the percentage of patients who felt their concerns were dismissed or minimized from a subgroup analysis of McL survey respondents who had experienced, or are experiencing, infertility or miscarriage.
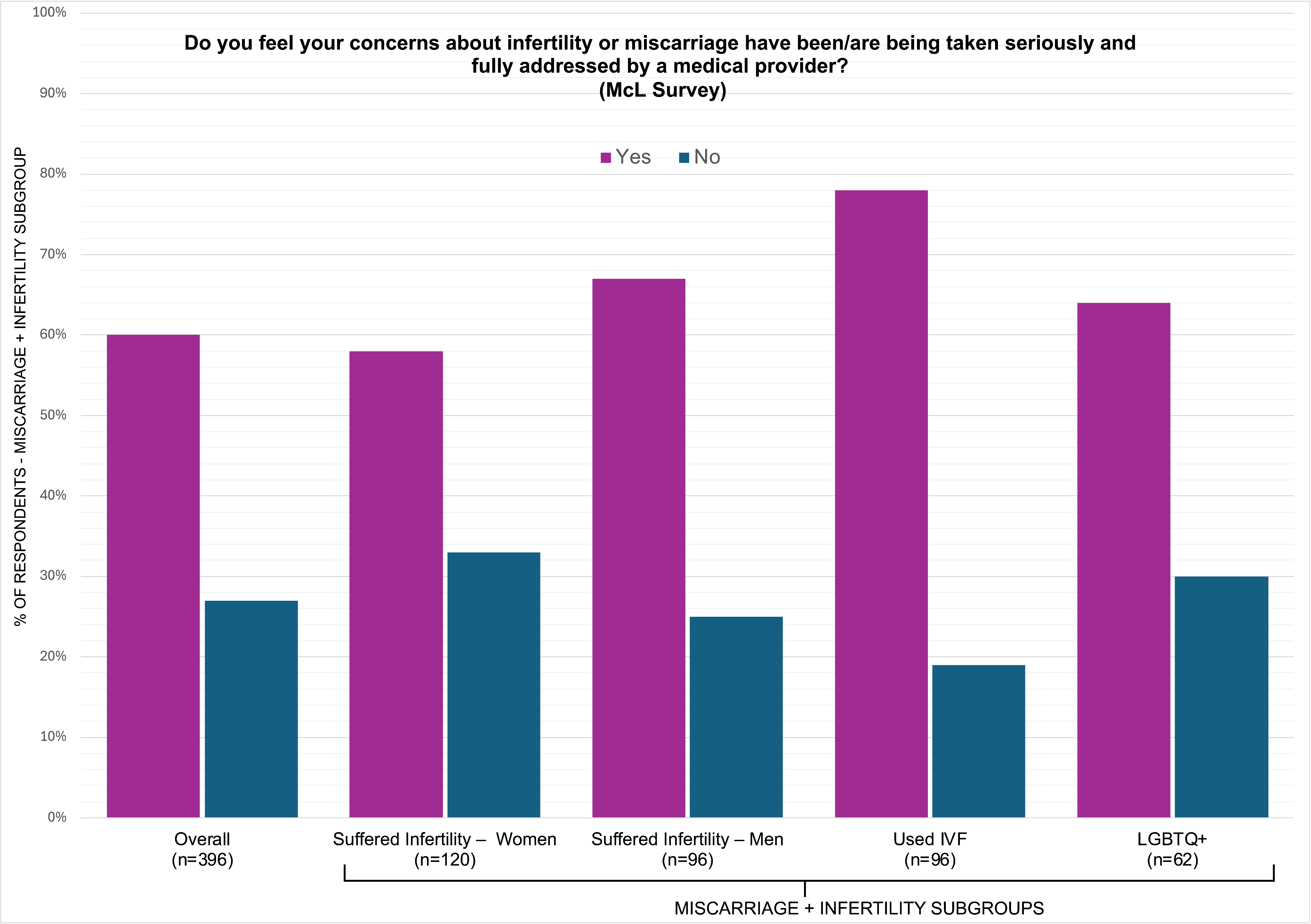
Figure 11. Patient perception of whether their concerns about infertility or miscarriage were taken seriously based on a subgroup analysis of McL survey respondents who had experienced, or are experiencing, infertility or miscarriage.
When asked whether they felt “fast-tracked” or pressured to consider IVF before other treatments were tried, 57% of those who had undergone IVF reported feeling fast-tracked to IVF. By comparison, among respondents with a history of infertility or miscarriage who had not undergone IVF, 9& (n=298) reported feeling fast-tracked to IVF.
Knowledge of IVF, attitudes toward medical risks, embryo selection and storage, and informed consent
JLP Survey
When asked to identify the correct definition of in vitro fertilization (IVF), only 564 of 1,002 respondents (56%) in the JLP survey selected the correct answer, which defined IVF as “a fertility treatment where eggs are fertilized with sperm in a laboratory, and the resulting embryo(s) are then transferred to the woman’s uterus to grow and develop.” These results indicate that nearly half of survey participants lacked accurate knowledge of IVF, highlighting potential gaps in understanding of fertility treatments.
Many survey questions also explored ethical issues and awareness of potential risks associated with IVF. Maternal risks of IVF pregnancies—including pre-eclampsia, gestational diabetes, severe maternal morbidity, and caesarean delivery—have been documented in the literature,18, 19, 2018, yet nearly half (49%) reported being unaware of any risks. A majority of respondents (77%) felt that risks to children conceived by IVF including premature birth, low birth weight, cancer, congenital heart defects and developmental issues were a factor in considering IVF, and that fertility specialists needed to do more to inform women about the potential risks before treatment (55%).21, 22 There was an overwhelming support for transparency and standardization in how IVF clinics report their data (73%).
Questions also explored embryo use, including creation for research, number created, preimplantation genetic diagnosis, and disposition of unused embryos. Nearly half (44%) of respondents felt there should be limits on the number created and 54% supported regulation that all embryos must eventually be implanted. 61% of respondents were unaware that IVF clinics offer preimplantation genetic testing (PGT) to screen embryos for various factors, including genetic conditions and sex selection. 35% believed that selecting for sex or intelligence should not be permitted (43% in favor; 22% unsure), and 48% supported regulations to restrict this practice.
Opinions varied in what should be done for embryos no longer required (Figure 12). There was also support endorsed for increased government regulation of IVF clinics and practices, including removing anonymous gamete donation (50%), limits on sperm donors (66%), and limits on creating embryos just for research purposes (63%).
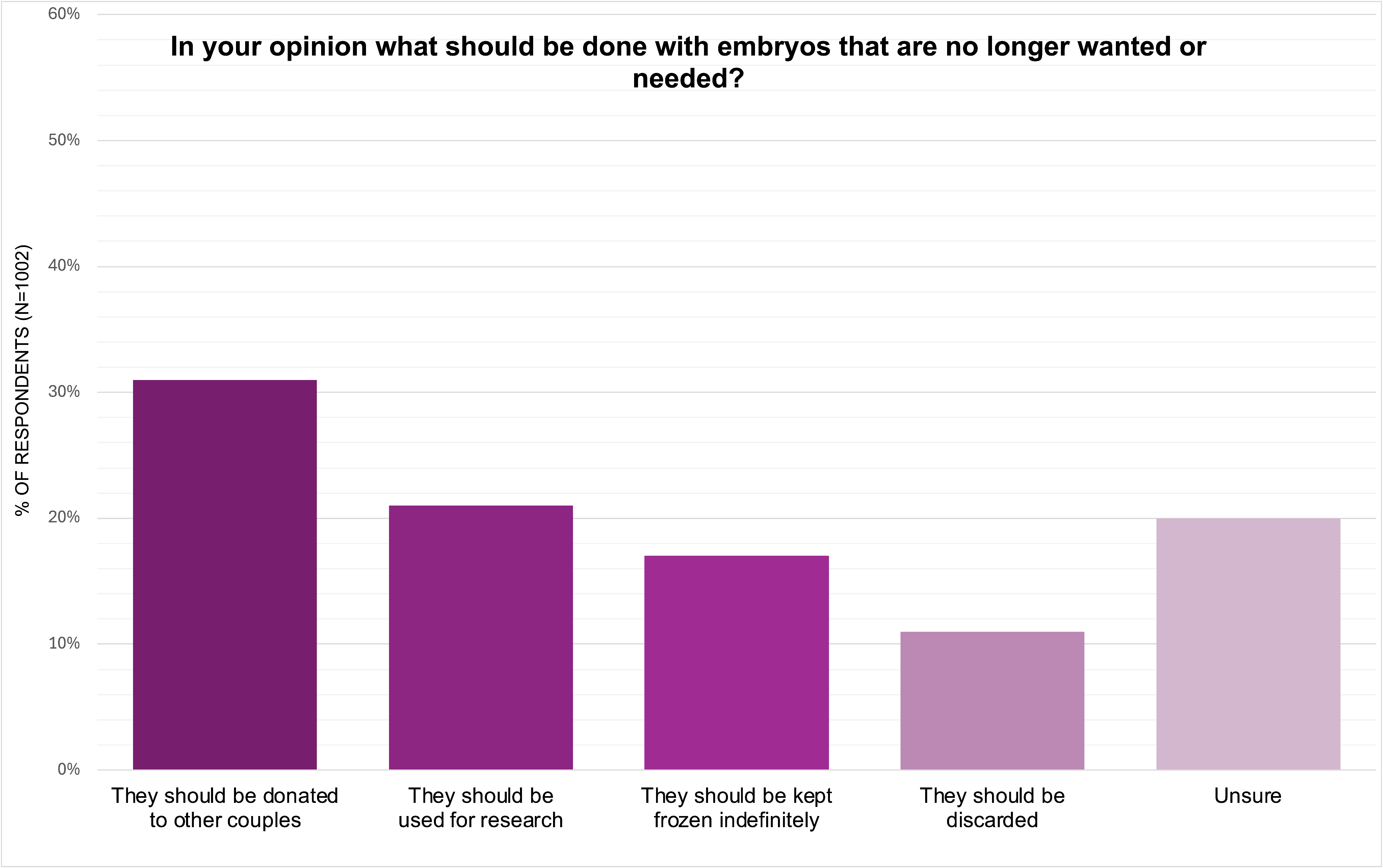
Figure 12. Responses from the JLP survey (N=1002) when participants were asked what should be done with embryos that are no longer wanted or needed.
McL Survey
In the McL survey, respondents overwhelmingly felt it was important to provide information on all medically sound options (84%, n=842) and possible negative outcomes. When asked how important it was for patients to receive information about “possible concerning ethical issues” when deciding on fertility treatment, 77% (n=769) of respondents felt that patients should receive information on these, with 54% (n=541) feeling very strongly, and 23% (n=229) feeling it was somewhat important. 14% felt it was not important (n=137) and 9% (n=94) did not answer the question.
DISCUSSION
This paper explores attitudes toward RRM and IVF through a secondary analysis of two nationally representative U.S. surveys. The findings underscore the prevalence of infertility and miscarriage and their widespread impact on U.S. adults.23 Since the 1970s, reproductive medicine has evolved toward two very differing approaches to reproductive health. The more commonly known approach of ART (assisted reproductive technologies), which centers on IVF, focuses primarily on the outcome of a pregnancy and live birth, while often bypassing the underlying causes of infertility; the other, restorative reproductive medicine (RRM), focuses primarily on diagnosing and treating the underlying pathology, with pregnancy and live birth as an expected outcome for those seeking it.24
While IVF remains the most recognized fertility treatment, even the basic details of it were not well understood by many survey respondents. In contrast, the term RRM was not recognized by most respondents. However, most respondents expressed a preference for restorative approaches when these were described for them. In hypothetical scenarios, there was a strong preference for natural fertilization within a woman’s body (Figure 5) and prioritizing healthy outcomes (Figure 4 and Figure 8). After naming and defining both RRM and IVF, specifically, approval of both approaches was high and similar for most subgroups (Figure 7). This preference suggests strong public interest in fertility treatments that focus on improving overall reproductive health. Limited awareness of RRM presents an opportunity for health care professionals to educate patients about options for RRM treatment modalities.
Although most patients would be eligible for either treatment option, robust comparative efficacy studies are lacking. RRM requires functioning or repaired male and female reproductive organs and the ability to complete the act of intercourse. RRM does not utilize gamete or embryo transfer, while IVF does. Both RRM and IVF (using autologous oocytes) achieve fewer pregnancies in older women, those with longer established infertility, and those with higher body mass indices, and both require a functional uterus. According to available data, success rates for either approach seem comparable for couples with infertility who are eligible for either approach. 10, 11. 12, 13 Further, even after IVF failure, many patients can achieve successful, healthy pregnancies with RRM.14
The respondents’ prioritization of infant health over speed or cost further reflects patient-centered values in treatment decision-making.25, 26 Patient-centered models of care that emphasize diagnosis, ongoing evaluation, and health restoration -- hallmarks of RRM -- may be well aligned with many public and patient preferences, particularly among individuals who perceive IVF as procedurally demanding or lacking transparency in clinical processes.
While large majorities felt their concerns about miscarriage or infertility were addressed by a medical provider, 83% of IVF patients remain concerned that an underlying diagnosis was missed. This challenges the perception that IVF resolves infertility as a medical condition. The surveys reveal that over half of patients, particularly women and LGBTQ+ individuals, felt their symptoms were dismissed or minimized during fertility care, suggesting inadequate diagnostic evaluation and/or communication.
These findings echo qualitative research from the UK, where couples described IVF as a routine and almost inevitable step in fertility care, often offered with little investigation of underlying causes.27 Their accounts highlighted feelings of being rushed into treatment, limited choice of alternatives, and ongoing uncertainty described as “mazing,” or a recursive pursuit of parenthood. Similar concerns have been raised by Kamphuis et al., who caution that IVF is increasingly applied to unexplained or mild subfertility without robust evidence of benefit.28 Their analysis suggests that many couples may conceive naturally with a longer period of expectant management, potentially avoiding the medical risks and costs associated with IVF.
Also notable in the JLP survey was the shift in attitudes toward IVF after participants were presented with information regarding medical risks to mother and fetus or neonate, the creation and use of embryos associated with IVF, and options for government regulation. Support for IVF decreased from 82% to 71% following this information. However, it is difficult to present such information completely and accurately in a survey format and the wording of the questions in the survey can be perceived as leading toward a desired response.
STRENGTHS AND LIMITATIONS
A strength of this study is the large, demographically representative U.S. samples, which included both individuals with and without direct infertility experience. The use of two independent surveys and use of validated survey methods provided complementary perspectives and increased robustness of the findings. Limitations include reliance on self-reported data, which are subject to recall and response bias, and the inability to link individual pre- and post-survey responses. Some, but not all, survey items included “don’t know” or “refuse to answer” response options, making comparisons with items lacking these options difficult.
The surveys were commissioned by organizations engaged in reproductive health policy and advocacy. While these datasets provide valuable insights into public perceptions, the potential for framing effects aligned with commissioning priorities represents an inherent limitation of secondary analysis of externally designed surveys. In addition, the wording of some questions may have influenced responses.
Interestingly, the proportion of respondents with reported infertility experience (22 %) was higher than U.S. population estimates (9-15%), and global estimates reported by the World Health Organization.29, 30 This may suggest that individuals with infertility experience were more likely to participate in the surveys and/or potential differences in how history of infertility was defined or assessed across surveys. In addition, the medical risks described in the JLP survey in question regarding adverse reproductive health outcomes were not quantified, which may have influenced respondents’ opinions.
The surveys did not ask which type of clinicians the respondents had consulted; therefore, the specialty or training of the providers is unknown. This limits interpretation of the questions about experiences with diagnosis and treatment. As both surveys were limited to U.S. adults, findings may not be generalizable to other populations.
CONCLUSION
The J.L. Partners and McLaughlin surveys provide important insights into reproductive health experiences and attitudes among U.S. adults. The findings suggest that RRM may align with the values and diagnostic expectations of many individuals with infertility. Respondents expressed strong interest in approaches that prioritize identifying and treating underlying health factors contributing to infertility and that emphasize the health of the baby. They also endorsed greater transparency to better understand all treatment options, including the potential health risks associated with treatments.
These findings highlight the need for increased education on RRM and a broader health care emphasis on prevention and restorative approaches. The results also underscore the importance of considering patient and public treatment preferences in fertility care. Continued national surveys are warranted to monitor trends and inform clinical and public health strategies. A more expansive, patient-centered regulatory framework including expanded access to RRM may help address unmet needs and concerns that persist in contemporary fertility care.
FUNDING STATEMENT
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
DISCLOSURE STATEMENT
Tracey Parnell serves as Managing Editor of the Journal of Restorative Reproductive Medicine (JRRM). Kathleen Copeland provides technical and systems support for JRRM.
These roles had no influence on the study design, analysis, interpretation of data, or decision to submit for publication. The authors were not involved in the editorial review or decision-making process for this manuscript. The authors declare no other competing interests.
ETHICS APPROVAL
This study met the requirements for institutional review board exemption as per Tri-Council Policy Article 2.4 (https://ethics.gc.ca/eng/tcps2-eptc2_2022_chapter2-chapitre2.html). It is a secondary analysis of anonymized, aggregate data from two previously conducted surveys. Participant information was recorded in such a manner that the human subjects involved cannot be identified.
AUTHOR CONTRIBUTIONS
TP: Conceptualization, Formal analysis, Visualization, Investigation, Writing – original draft, review & editing. KC: Formal analysis, Statistical Analysis, Visualization (graphs), Writing – review & editing. MM: Writing – review &editing. All authors read and approved the final manuscript.
DATA AVAILABILITY STATEMENT
The data reported in this article include publicly available survey results as well as raw data from the McL survey provided to the authors by the survey investigators. Raw McL survey data are available from the corresponding author upon request.
REFERENCES
- WHO. Infertility. Available from: https://www.who.int/news-room/fact-sheets/detail/infertility. Accessed: May 23rd, 2023.
- Thoma ME, McLain AC, Louis JF, King RB, Trumble AC, Sundaram R, Buck Louis GM. Prevalence of infertility in the United States as estimated by the current duration approach and a traditional constructed approach. Fertil Steril. 2013 Apr;99(5):1324-1331.e1. doi: 10.1016/j.fertnstert.2012.11.037. Epub 2013 Jan 3. PMID: 23290741; PMCID: PMC3615032.
- Snow M, Vranich TM, Perin J, Trent M. Estimates of infertility in the United States: 1995-2019. Fertil Steril. 2022 Sep;118(3):560-567. doi: 10.1016/j.fertnstert.2022.05.018. Epub 2022 Jun 14. PMID: 35710598.
- Deyhoul N, Mohamaddoost T, Hosseini M. Infertility-Related Risk Factors: A Systematic Review. Int J of Women’s Health Reprod Sci. 2017 Jan;5(1):24-29. doi: 10.15296/ijwhr.2017.05.
- Henrich N, Jahnke HR. 2025. Mental Health Across the Conception Journey: Trying To Conceive Without Treatment, Considering Treatment, and with Treatment. Matern Child Health J. 2025 Oct;29(10):1360-1365. doi:10.1007/s10995-025-04157-9. Epub Sep 9. PMID:40926166; PMCID: PMC12484304.
- Steptoe PC, Edwards RG. Birth after the reimplantation of a human embryo. Lancet. 1978 Aug 12;2(8085):366. doi:10.1016/S0140-6736(78)92957-4. PMID: 79723.
- Yovich JL, Craft IL. Founding Pioneers of IVF: Independent innovative researchers generating livebirths within 4 years of the first birth. Reprod Biol. 2018 Dec;18(4):317-323. doi: 10.1016/j.repbio.2018.11.004. Epub 2018 Dec 1. PMID: 30509752.
- Dyer S, Chambers GM, Jwa SC, Baker V, Banker M, de Mouzon J, Elgindy E, Fu B, Ishihara O, Kupka MS, ZegersHochschild F, Adamson GD, International Committee for Monitoring Assisted Reproductive Technologies world report: assisted reproductive technology, 2019, doi: 10.1016/j.fertnstert.2025.06.003.
- Adamson GD, Creighton P, de Mouzon J, ZegersHochschild F, Dyer S, Chambers GM. How many infants have been born with the help of assisted reproductive technology? Fertil Steril. 2025 Jul;124(1):40-50. doi:10.1016/j.fertnstert.2025.02.009. Epub 2025 Feb 11. PMID:39947276.
- Boyle P. Understanding Restorative Reproductive Medicine. Journal of Restorative Reproductive Medicine. 2025 Sept 17; 1:7:1-2. https://doi.org/10.63264/f0b0xh81
- Stanford JB, Carpentier PA, Meier BL, Rollo M, Tingey B. Restorative reproductive medicine for infertility in two family medicine clinics in New England, an observational study. BMC Pregnancy Childbirth. 2021 Jul 7;21(1):495. doi: 10.1186/s12884-021-03946-8. PMID: 34233646; PMCID: PMC8265110
- Sanchez-Mendez JI, Lombarte M, Abengozar-Muela R, Acosta-Diez J, Alonso-Fernandez P, Canones-Castanon MP, Calderon-Ruiz O, Espinosa-Garcia E, GalochaMorgado C, Siegrist J et al. Natural procreative technology (NaProTechnology) for infertility: take-home baby rate and clinical outcomes in a 5-year single-center cohort of 1,310 couples. Front Reprod Health 2025;7: 1696679. doi: 10.3389/frph.2025.1696679.
- Boyle PC, de Groot T, Andralojc KM, Parnell TA. Healthy Singleton Pregnancies From Restorative Reproductive Medicine (RRM) After Failed IVF. Front Med (Lausanne). 2018 Jul 31;5:210. doi:10.3389/fmed.2018.00210. PMID: 30109231; PMCID: PMC6079215.
- Boyle P, Toth A, Minjeur M, Turczynski C. 2025. Restorative reproductive medicine (RRM) outcomes compared to in-vitro fertilization (IVF) for the treatment of infertility: a retrospective evaluation of a 2019 clinic cohort compared to one cycle of IVF. J Restorative Reprod Med [Internet]. Sep. https://doi.org/10.63264/gejytw70.
- The Heritage Foundation, J.L. Partners. Americans’ knowledge of and opinions about in vitro fertilization (IVF) [Internet]. Washington (DC): The Heritage Foundation; 2025. Available from: https://static.heritage.org/-2025/IVF_Poll.pdf.
- Women's Reproductive Health Foundation. National Infertility Experience Survey [Internet]. womensrhf.org.2025 [cited 2026 Mar 8]. Available from: https://www.womensrhf.org/ [Special Projects].
- Bureau UC. Census.gov | U.S. Census Bureau Homepage [Internet]. Census.gov. 2025 [cited 202 Infertility prevalence estimates, 1990–2021. Geneva: World Health Organization; 2023. License: CC BY-NC-SA 3.0 IGO 5 Aug 22]. Available from: https://www.census.gov/
- Sunderam S, Kissin DM, Zhang Y, et al. Assisted Reproductive Technology Surveillance — United States, 2018. MMWR Surveill Summ 2022;71(No. SS-4):1–19. doi: 10.15585/mmwr.ss7104a1.
- Belanoff C, Declercq ER, Diop H, Gopal D, Kotelchuck M, Luke B, Nguyen T, Stern JE. Severe Maternal Morbidity and the Use of Assisted Reproductive Technology in Massachusetts. Obstet Gynecol. 2016 Mar;127(3):527-534. doi: 10.1097/AOG.0000000000001292. PMID: 26855105; PMCID: PMC4764424.
- Vaajala M, Liukkonen R, Ponkilainen V, Mattila VM, Kekki M, Kuitunen I. In vitro fertilization increases the odds of gestational diabetes: a nationwide register-based cohort study. Acta Diabetol. 2023 Feb;60(2):319-321. doi: 10.1007/s00592-022-01975-z. Epub 2022 Oct 22. PMID: 36271972; PMCID: PMC9852144.
- Reeder MR, Stanford JB, Porucznik CA, Schliep KC, Johnstone E, Botto LD, Hotaling J. Neonatal characteristics of children conceived with in vitro fertilization or intrauterine insemination compared with sibling births from unassisted conceptions. Fertil Steril. 2026 Feb;125(2):326-337. doi: 10.1016/j.fertnstert.2025.08.027. Epub 2025 Aug 26.
- American College of Obstetricians and Gynecologists’ Committee on Obstetric Practice; Committee on Genetics; U.S. Food and Drug Administration. Committee Opinion No 671: Perinatal Risks Associated With Assisted Reproductive Technology. Obstet Gynecol. 2016 Sep;128(3):e61-8. doi: 10.1097/AOG.0000000000001643
- Thoma ME, McLain AC, Louis JF, King RB, Trumble AC, Sundaram R, Buck Louis GM. Prevalence of infertility in the United States as estimated by the current duration approach and a traditional constructed approach. Fertil Steril 2013;99: 1324–1331. doi: 10.1016/j.fertnstert.2012.11.037.
- Arraztoa JA. Commentary on infertility and restorative reproductive medicine. J Restorative Reprod Med 2025:1;1–5. doi: 10.63264/7eg52623.
- Gusmano MK, Maschke KJ, Solomon MZ. PatientCentered Care, Yes; Patients As Consumers, No. Health Aff (Millwood). 2019 Mar;38(3):368-373. doi:10.1377/hlthaff.2018.05019. PMID: 30830817
- Duthie EA, Cooper A, Davis JB, Schoyer KD, Sandlow J, Strawn EY, Flynn KE. A conceptual framework for patient-centered fertility treatment. Reprod Health. 2017 Sep 7;14(1):114. doi: 10.1186/s12978-017-0375-5. PMID: 28882134; PMCID: PMC5590184.
- ounce G, Allan HT, Carey N. 'Just have some IVF!': A longitudinal ethnographic study of couples' experiences of seeking fertility treatment. Sociol Health Illn.2022;44(2):308-327. doi:10.1111/1467-9566.13429
- Kamphuis EI, Bhattacharya S, van der Veen F, Mol BW, Templeton A; Evidence Based IVF Group. Are we overusing IVF?. BMJ. 2014;348:g252. Published 2014 Jan 28. doi:10.1136/bmj.g252
- Infertility prevalence estimates, 1990–2021. Geneva: World Health Organization; 2023. Licence: CC BY-NC-SA 3.0 IGO. Available from: https://www.who.int/publications/i/item/978920068315.
- National Center for Health Statistics. Cdc.gov. Published March 17, 2025. Accessed August 22, 2025. https://www.cdc.gov/nchs/fastats/infertility.html
Correspondence to: Tracey Parnell.
Email: drparnell@iirrm.org
How to cite this article: Parnell T, Copeland K, Minjeur M. Public Awareness, Perceptions, and Preferences in Fertility Treatment: Secondary Analysis of Two Public Surveys. J Restorative Reprod Med. 2026 April 15, 2:2 1–20. https://doi.org/10.63264/6yy3mw82
COPYRIGHT
© The Author(s) 2026. Published by the Journal of Restorative Reproductive Medicine. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International Licence, which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium, provided the original work is properly cited.
Received: November 29, 2025; Revised: April 14, 2026, 2025; Accepted: April 15, 2026. Published: April 15, 2026.
